Constipation is a common problem in children causing 5% of the visits to the pediatrician and 30% of visits to the gastroenterologist.
In children older than 1 yr of age 95% of the cases its cause is functional, and only 5% of them have an organic cause
.It is important to address this issue when young because 25% of children with constipation will continue to have issues into adulthood.
How does it all work?
The transit of the colon works in response to intestinal contractions. In infants these can happen 6-7 times a day and happen even at rest. As kids get older they decrease in frequency. The most common one happens in response to a meal and distention of the stomach... "the gastrocolic reflex".
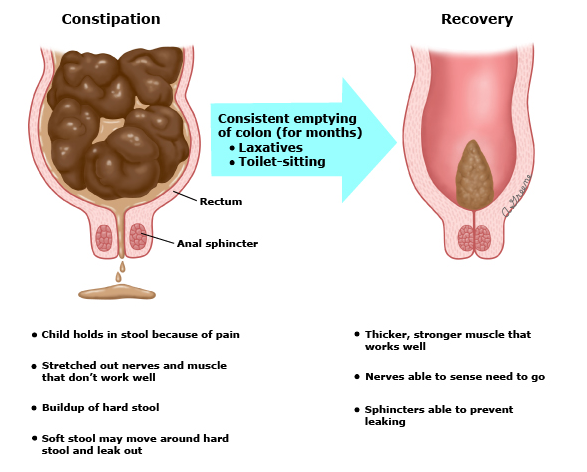
As the rectum, the last part of the colon, fills up with stool and gets distended, the sensation or urge to have a BM is created.
The colon is an elastic organ, and like a "scrunchy" as it gets stretched or distended, it looses it's elasticity and the fibers can't contract as effectively. This causes loose of sensation or "urge" and weaker muscles.
The rectum job is to reabsorb water from the stool while it is there, and it continues to do so even when the stool has been there for a few days, making the stool harder and larger.
The combination of larger and harder stools, with weaker rectum muscles and lower sensation, and with the same size anus causes pain when having a BM, trauma and holding behavior.
Stool accidents can be of 2 types:
- younger child who is spending most of the time holding the stool, the moment they relax a small amount of formed stool comes out.
- older kids who are impacted with large stool and do not completely empty the rectum, liquid stool can seep through without them being aware that it is happening.
Treatment and rehabilitation can restore normal colonic function but in order to be successful every part of the cycle has to be addressed.